
This post summarises a note I have drafted on the definition of “transformative WASH”, available here, with references.
There has been a lot of talk about “transformative” WASH since the WASH-B, SHINE and MapSan results came out. I have previously written about those results here. The argument runs that “basic” or “elementary” WASH services do not reduce environmental faecal contamination to a sufficient degree to see health impact, so we need transformative interventions. However, authors typically provide little detail on how they see “transformative WASH”, which is unsurprising for an emerging concept.
In the note, I summarise what has been written about transformative WASH, adding reflections and an economic evaluation perspective. What emerges from existing publications is an idea of transformative WASH as “safely-managed” levels of water and sanitation service in combination with basic hygiene, better housing conditions (e.g. sealed floors / play spaces) and better management of animals, all with a view to reduced faecal contamination and health gains. Most authors also agree that the WASH system functions such as policy, planning, M&E and regulation are important enabling factors for transformative WASH.
I have five points to make:
1. I tend to think of “transformative” as a level of ambition, rather than a level of service. Being transformative, then, is about achieving incremental changes which are large rather than small, regardless of the starting point or end point.
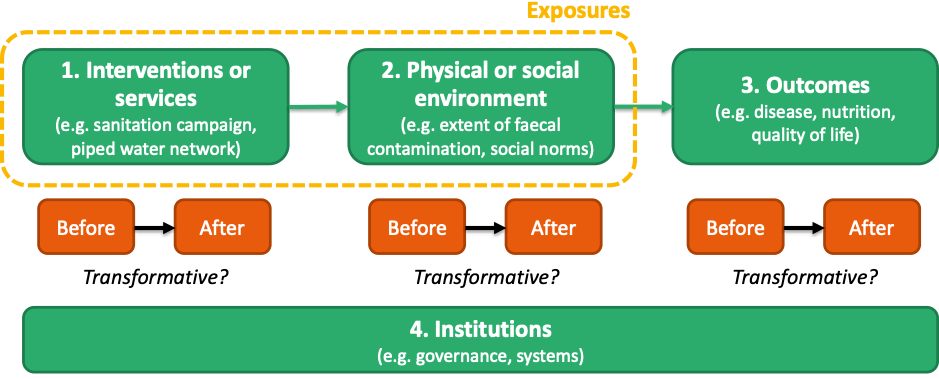
2. I also tend to think about transformation in terms of outcomes, as opposed to interventions or environmental contamination (Figure 1). By outcomes I mean not only infectious disease and nutrition, but also quality of life, because users value WASH services for many reasons.
3. As and when a definition emerges, it does not follow that only interventions which are “transformative” in disease risk terms should be funded. The most economically efficient interventions are not necessarily those which are most effective at improving health. The costs of a highly effective intervention may be substantially higher than the next best option, to the extent that it is much less cost-beneficial. Choosing the most efficient interventions permits extending services to a larger number of people within a given budget constraint, maximising net benefits to society.
4. The equity principle demands that a substantial proportion of collective effort is placed on extending services to those with the worst levels of service at present.
5. To avoid wasted investments, services must be sustained. Recurrent costs typically increase with level of service, and must be covered. Therefore, levels of service offered should be aligned with households’ willingness and ability to pay those recurrent costs. Without this principle, services may fall into disrepair or low levels of uptake will make schemes inefficient to run.
This post summarises a note (available here), which summarises what has been written about transformative WASH, adding reflections and an economic perspective. I summary, I see “transformative” as a level of ambition, rather than a level of service, best conceptualised at the level of outcomes. Being transformative is then about achieving incremental changes which are large rather than small, regardless of the starting point or end point. The most economically efficient interventions are not necessarily those which are most effective in health terms.
